
Donate to Nurses Talk Healthcare in America
GALLUP RANKS NURSES #1 IN HONESTY, ETHICS, 16 OF PAST 17 YEARS There’s never been a better time for nurses to have a national media presence. With an 85% honesty and ethics rating from Gallup Poll’s annual ranking of how Americans view 21 major professions—nurses […]

Shopping Abroad For Cheaper Medication? Here’s What You Need To Know
In its effort to temper the sky-high prices Americans pay for many vital medications, the Trump administration last month unveiled a plan that would legalize the importation of selected prescription drugs from countries where they sell for far less. But the plan addresses imports only at the […]
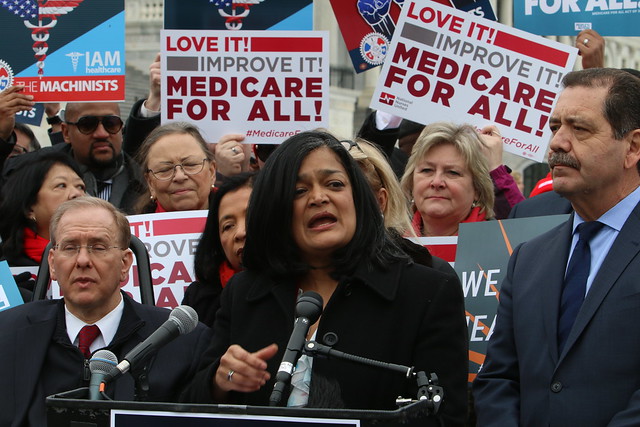
It’s time for Democrats to get their facts right on Medicare-for-all
By Pramila Jayapal, a Democrat, representing Washington’s 7th Congressional District in the U.S. House. In the wake of the second Democratic presidential debate, it is clear that Medicare-for-all has become a defining issue of the 2020 election. Earlier this year, when I introduced our comprehensive, […]

Nurses Challenge Climate Change
The Nurses Climate Challenge is a national campaign to mobilize nurses to educate 50,000 health professionals on the impacts of climate change on human health. Health care is at the frontline of climate change, bearing the costs of increased disease prevalence and more frequent extreme […]

A Salute to Nurses with Jane O’Meara Sanders
We need to stand by the nurses. We need to support them. We need to support their unions and we need to provide Medicare for all especially.” –Jane O’Meara Sanders Nurse Talk’s Healthcare in America Senior Correspondent Donna Smith had the privilege of talking with […]

Is It Possible to Change a Habit in Seven Days? Hypnotherapist Georgia Foster Says Yes.
Clinical Hypnotherapist Georgia Foster has been a long sought-after expert commenter on the subject of how to drink less in her home country of Australia, and in the UK where she now lives. Georgia is a world-leading therapist, specializing in overdrinking behavior (as well as […]

A Decision to be of Service
Dr. Grace Dammann’s life was forever altered when a driver crashed head-on into her car on the Golden Gate Bridge. Dr. Dammann once honored by the Dalai Lama for her extraordinary work with AIDS patients’ said, “It’s a real eye-opener to be on the other side […]

Nurse Talk heard on the Thom Hartmann Program | Nurses say Medicare for All, not about politics, its about patients
As nurses in our practice we see the lack of preventative healthcare and what that leads to for outcomes. This is an exciting light at the end of the tunnel so our patients will be cared for and our communities will be healthier. — RN […]

DANGER IN DISGUISE…why nurse licensure compact seems like a good idea BUT not so fast!
Ask yourself, who do you trust to make decisions about who should be allowed to practice nursing in your state? Do you trust your state’s nursing board, or would you trust an organization with little oversight and a comfy relationship with corporate sponsors such as […]